TMJ, TMD and Orofacial Pain are terms that you commonly hear or read in relation to pain and other symptoms related to the head and neck, but what do they really mean?
There is a lot of confusion about these terms. They are commonly, and wrongly, used interchangeably. Sadly, many dentists are at least partly responsible for this confusion, because, for the sake of convenience or simplicity, it is easier to just use the first term that comes to mind. But this is lazy and misleading.
Defining the terms.
So, let’s look at these terms and their real meaning.
TMJ – is the acronym of Temporomandibular Joint.
…and that it all it is. The TMJ is a joint. “TMJ” is not a disease, distortion or condition, even though it is sometimes wrongly used in that way.
TMD – is the acronym for the condition called Temporomandibular Joint Dysfunction (or Disorder).
This is a condition where the TMJ is not functioning properly, and commonly involves muscles, bones and cartilege associated with the joint and its function
Orofacial Pain – is a much broader condition involving any form of Pain involving the Mouth (Oro-) and Face (-Facial).
This can include pain associated with the TMJs and includes many of the symptoms of TMD. But includes other pains and sources of pain.
So let’s look at these terms in more detail.
TMJ.
The Temporomandibular Joint is located just in front of the ear.
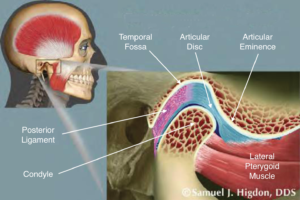
From the image –
- The Temporal Fossa is in the Temporal bone on the base of the skull.
- The Condyle is at the top of the Mandible.
- The Articular Disc offers protection of the bones. It acts to some extent as a shock absorber between the bones, as well as easing the movement of the bones in relation to each other.
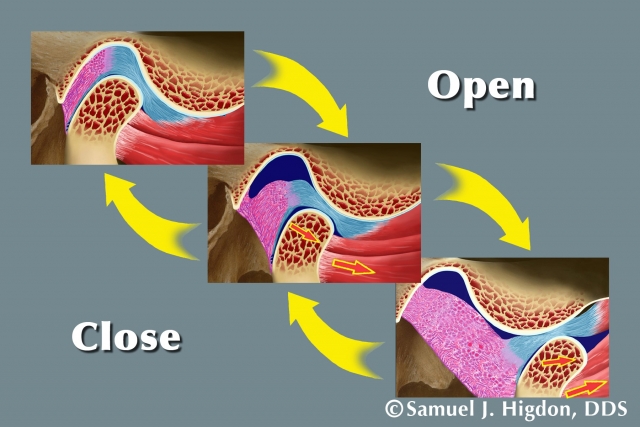
- The Lateral Pterygoid muscle is the main muscle involved in moving the Condyle and Disc forward along the Articular Eminence during mouth opening, and moving the jaw side to side in chewing or grinding the teeth.
The areas of bone subjected to the greatest force during normal function are the antero-superior (frontand top) part of the condyle, and the Articular Eminence. The Disc is always positioned in between the bones. The Condyle rotates against the lower surface of the Disc, and the upper surface of the Disc slides against the Articular Eminence.
TMD.
This occurs when there is a Disorder or Dysfunction of the TMJ.
A Disorder of the joint describes when the structures of the joint ore out of order or out of their correct position. This is best described as a disturbance in the Condyle/Disc/Fossa relationships. This is most commonly found in joint radiographs where the Condyle is out of the correct position in the Fossa. It is typicaly too far back or back and up, but occasionally in other directions as well.
A Dysfunction of the joint is when it is not functioning properly. This is seen in the clinic when the condyle is not moving far enough, or is moving irregularly, or when both condyles are not moving in harmony – which means the lower jaw typically wriggles a little on opening.
TMD is a very big subject with wide ranging symptoms – way too big to discuss in any blog post.
I have given more information about TMD in my post here –
I discuss the major cause of TMD here –
Orofacial Pain
Orofacial Pain – refers to any pain of the mouth or face. It can include such things as toothache, muscle problems, TMD, trauma, cancer and neurological problems.
The International Headache Society has published the “International Classification of Orofacial Pain”, which classifies by the category of pain and its causes –
- Orofacial pain attributed to disorders of dentoalveolar and anatomically related structures – teeth, gums and their supporting bone are the source of the pain.
- Myofascial orofacial pain – Muscle based problems – but the classification makes no allowance for the fact that muscles don’t become painful without a reason – something else is actually causing the muscle problem.
- Temporomandibular joint (TMJ) pain – this is one aspect of TMD. It only refers to pain from the joints themselves, and ignores all of the other joint-related problems like myofascial problems.
- Orofacial pain attributed to lesion or disease of the cranial nerves – this is truly a neurological problem and includes Trigeminal Neuralgia (the most common of these types of Orofacial Pain)
- Orofacial pains resembling presentations of primary headaches – Primary Headache means a headache which has no other cause, but the description of this class of Orofacial Pain goes on to describe neurological, vascular and neurovascular headaches – which are not actually “Primary”. This is a strange category.
- Idiopathic orofacial pain – In medicine, if something is “Idiopathic”, this simply means that nobody has yet found the actual cause of the problem. So pretty much anything that the doctor can’t explain is thrown into this category.
- Psychosocial assessment of patients with orofacial pain – Another strange category, which is not actually a pain problem or the cause of pain. This section only discusses the way to assess any social, psychological or other environmental factors which might contribute to pain.
Some dentists are very quick to put their patients into the Psychosocial category, and prescribe pain medication, Botox, and psychological counselling. It is much easier for them, but it doesn’t address them more common causes. In over four decades of treating Orofacial Pain, I have never, yet, seen a patient whose problem was caused by Psychosocial problems. Social and emotional stresses certainly contribute to pain, but I have not yet seen anyone for whom these stressors were the cause.
In fact, many of the patients I have seen have certainly suffered from depression and anxiety. but these problems have been the result of chronic pain, not the cause. by treating the cause of their pain problems, their depression and anxiety melt away, as the pain is no longer causing their depression.
(I know I will be criticised for the previous two paragraphs by those who are convinced that most Orofacial Pain is of psychosocial origin. But in reality, if you show me an Orofacial Pain patient, I will find a source of their problem other than stress. Once that source is addressed, the stress goes away.)
In more than four decades, I have never yet seen a patient for whom I was unable to track down the cause – which, in some cases, needed other specialists to correct.
What is Most Common?
In my experience, almost all of the Orofacial patients I have seen have had a TMD. Of the others –
- Four have had brain tumours – and my cranial nerve exam has allowed me to identify that they had intra-cranial lesions and I referred them off to the neurosurgeon
- A few have had other neurological problems
- Some have had vascular problems, neuromuscular problems or infections – all to be treated by Medical Specialists
- A number have had bite problems associated with improper development of the jaws, causing muscle pain, without any apparent TMD
Of the thousands ot Orofacial Pain patients I have seen, there were only about 20 who did not have either a TMD or a Bite-related problem for me to help them with.
Special Thanks to Dr Samuel J Higdon DDS for his permission to use his images.